
Stroke Recovery Revolution: The Effect of MSCs, MSC/EPO, and EPO3 on Arterial Ischemic Stroke Induced Rodents
By Neha Sharma
Stem cell research is a relatively new field, only emerging in the past 25 years. Since its emergence, many questions have been raised about how this amazing technology can potentially treat virtually any disability or disease. Stem cells, or cells derived from human embryonic cells, have the potential to differentiate into any type of cell in the body (depending on what type of stem cell it is). We are born with many stem cells, but as we grow, we lose more and more of them. An example of the usage of stem cells includes treating burnt skin, as stem cells can help promote skin growth by differentiating into specific skin cell types. Another common example would be bone marrow transplants to aid in creating new blood cells after radiation therapy. Essentially, stem cells serve as the foundation of every tissue in the human body, therefore becoming a tool to produce tissue in the lab. This opens up possibilities for many other uses, extending even to neuroscience.
One in 2000 newborn babies experience the phenomenon of neonatal stroke. The most common type of this stroke is arterial ischemic stroke. Stroke in general is characterized by the blockage of blood supply to a part of the brain, causing major cognitive and motor issues. Similarly, in the case of arterial ischemic stroke, there is a period where there isn’t enough blood flow in a specific part of the brain, causing reperfusion to follow, restoring the blood. This leads to increased excitotoxicity, reduced blood flow, and altered cell fate. Furthermore, the identification of neonatal stroke is quite difficult, often resulting in late diagnoses. Coupled with no currently accepted standard treatments, this study gives parents of children affected by the 1/2000 statistic hope. Researchers have stimulated an environment similar to arterial ischemic stroke. Using their model of the stroke, they injected three doses of erythropoietin (EPO3) during surgery in young rats. Erythropoietin is a hormone that stimulates the formation of blood cells, new neurons (neurogenesis), and new blood vessels (angiogenesis), while also exhibiting anti-inflammatory effects. Rats were also administered single doses of MSCs (mesenchymal stem cells), or MSCs preexposed to EPOs. MSCs are stromal cells that are associated with being highly plastic and their ability to aid in tissue differentiation. For each of the different experiments, the treatments were administered on day 3 or 7. These combined therapies offer hope for a new and effective treatment for victims of neonatal stroke.
The results show that the administered EPO3, MSC/EPO, and MSC did increase brain volume a few days after injury. For the standard MSC therapy, there was only subtle sensorimotor improvement and not many long-term cognitive/behavioral benefits. MSCs pre-exposed to EPO (MSC/EPO) exhibited cognitive enhancement, even if administered on day 7. Multiple doses of EPO improved brain volume long-term recognition and memory regardless if administered on day 3 or 7. This was the only treatment to improve exploratory behavior and reduce anxiety in adulthood, while most likely improving cognitive facets long-term. Therefore, future studies may include combining MSC/EPO and multiple doses of EPO to improve motor and cognitive function long-term.
I found this study to be enlightening and inspiring. Research that ties vasculature and brain organoid research is quite interesting, as it targets the creation of new blood vessels that help guide brain growth. This research lays the foundation for future work in this area in addition to raising a few questions about the prospective uses of EPO and MSCs outside of treating arterial ischemic stroke. Perhaps one day, this can be a standard treatment for treating all types of stroke and traumatic brain injury. But for now, almost 200 newborns worldwide, will be given a chance to live every day with the combined effort of EPOs and MSCs. What distinguishes the likelihood of surviving from that of dying is the quick differentiation of brain and blood cells aided by MSCs and EPOs. This study paves the way for more studies to investigate the applications of MSCs and EPOs while highlighting the importance of retaining cognitive/mental abilities.
Q/A with Dr.Gonzalez
Q: Why were the rodents killed on P63? Also, should another study be done to monitor the rodents till death, to figure out if there would be any other adverse effects?
A: We chose P63 because it is basically early adulthood. So it is the earliest reasonable time to look at long-term outcomes. You could keep them much longer, and we’ve gone as late as 6 months, but there is cost and effort associated with that so sometimes not worth it – plus we want to find out if a treatment worked so waiting 6 months is a long time. To determine adverse events, you should see them by then, but even if you don’t, you need a larger animal model (closer to human) to look at that.
Q: What exactly is happening at a cellular level to result in improvements when administered with MSCs?
A: We are looking now at what happens at a cellular level – to understand the mechanism of improvement. But you want to see if therapy worked before getting to the why, otherwise you are wasting your time.
Q: Why did you choose the specific timings of 3 and 7 days to administer them?
A: We chose Day 3 because we saw evidence of benefit with that time point before, but then wanted to push it later to see if there was still benefit, hence 3 days or 7 days. We previously saw benefit with 3 doses of EPO starting on day 7. The goal is determining delayed treatment strategy for stroke, and realistically most human babies wouldn’t be diagnosed until a few days in, so day 3 is the most reasonable early time point.
Q: Another recent neonatology trial administered EPOs, where it was given to a baby who had brain injury at birth, and it didn't help. Do you think it was because of the timing that it wasn't beneficial or maybe because EPOs are more associated with regeneration rather than limiting injury?
A: EPO+hypothermia didn’t work, short answer is we don’t know why, longer answer is that they work by similar mechanisms so no additive benefit, and there may be more benefit to EPO monotherapy given as delayed treatment for repair as opposed to reducing cell death, similar to what we did with these animals.
Read the original article here: https://www.ahajournals.org/doi/10.1161/STROKEAHA.120.031191
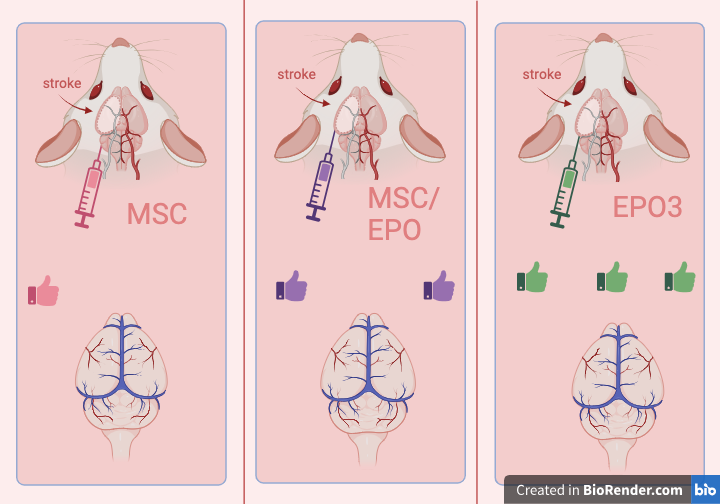
Figure: The combinatorial effects of MSCs and erythropoetin (EPO) after neonatal stroke.